Is Basal Cell Nevus Syndrome a cancer?
Basal cell nevus syndrome, or Gorlin syndrome, affects an estimated 1 in 31,000 people. Basal cell nevus syndrome raises your risk for a type of skin cancer called basal cell carcinoma. If you develop unusual spots or growths on your skin, let your healthcare provider know.
How would you describe basal cell carcinoma on a physical exam?
PHYSICAL FINDINGS—BASAL CELL CARCINOMAS The hallmark of basal cell carcinoma is a waxy, translucent, or pearly appearance. Commonly, these lesions have central ulceration and a raised pale border (Figure 2). The border may be highlighted by applying traction on the skin around the lesion (Figure 3).
How do you test for Gorlin syndrome?
Genetic testing
- An exam of the patient’s skin for basal cell carcinomas, pitting on hands and feet, areas of skin discoloration, and small cysts (milia) around the eyes and nose and elsewhere.
- An exam of the face and head to identify any abnormalities of the face, skull, teeth and jaws.
Is Gorlin syndrome genetic?
Gorlin syndrome is inherited in an autosomal dominant pattern, which means one copy of the altered gene in each cell is sufficient to cause the condition. In most cases, an affected person inherits the mutation from one affected parent .
Is Basal Cell Carcinoma inherited?
Inheritance and Risk Basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) are two of the most common malignancies in the United States and are often caused by sun exposure, although several hereditary syndromes and genes are also associated with an increased risk of developing these cancers.
What is basal cell nevus syndrome?
Basal cell nevus syndrome is an autosomal dominant condition with complete penetrance and variable expressivity. It is characterized by five major components, including multiple nevoid basal cell carcinomas, jaw cysts, congenital skeletal abnormalities, ectopic calcifications, and plantar or palmar pits.
How might you know you have basal cell carcinoma?
Basal cell carcinoma appears as a change in the skin, such as a growth or a sore that won’t heal. These changes in the skin (lesions) usually have one of the following characteristics: A shiny, skin-colored bump that’s translucent, meaning you can see a bit through the surface.
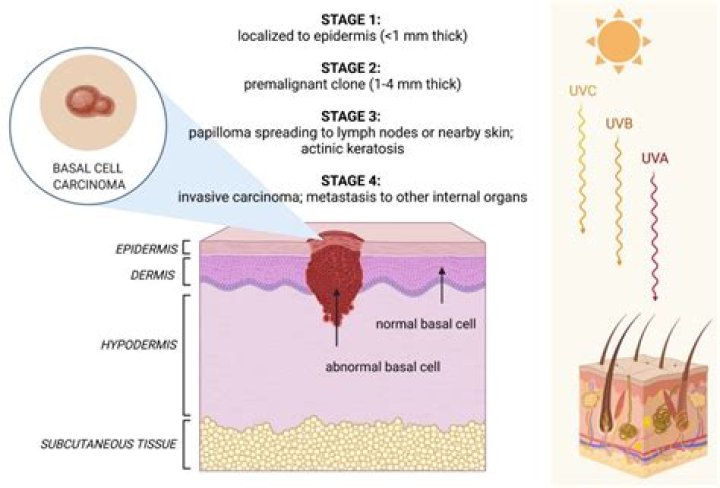
What are the clinical manifestations of basal cell carcinoma?
At first, a basal cell carcinoma comes up like a small “pearly” bump that looks like a flesh-colored mole or a pimple that doesn’t go away. Sometimes these growths can look dark. Or you may also see shiny pink or red patches that are slightly scaly. Another symptom to watch out for is a waxy, hard skin growth.
What is Muir Torre syndrome?
Muir-Torre syndrome (MTS) is a phenotypic variant of the hereditary nonpolyposis colorectal cancer (HNPCC) characterized by the association of sebaceous skin tumors and internal malignancies, most frequently colon cancer. It was first described by Muir et al1 in 1967 and then by Torre2 in 1968.
What are the diagnostic guidelines for basal cell nevus syndrome?
Basal Cell Nevus Syndrome: Guidelines for Early Detection. Basal cell nevus syndrome is an autosomal dominant condition with complete penetrance and variable expressivity. It is characterized by five major components, including multiple nevoid basal cell carcinomas, jaw cysts, congenital skeletal abnormalities, ectopic calcifications,…
What are the components of basal cell nevoid nevoid syndrome?
Basal Cell Nevus Syndrome: Guidelines for Early Detection. It is characterized by five major components, including multiple nevoid basal cell carcinomas, jaw cysts, congenital skeletal abnormalities, ectopic calcifications, and plantar or palmar pits. Other features include a host of benign tumors, ocular defects, and cleft lip and palate.
What is the prevalence of medulloblastoma in children with NBCCS?
Approximately 5% of all children with NBCCS develop medulloblastoma (primitive neuroectodermal tumor), generally the desmoplastic subtype. The risk of developing medulloblastoma is substantially higher in individuals with an SUFU pathogenic variant (33%) than in those with a PTCH1 pathogenic variant (<2%). Peak incidence is at age one to two years.